Treatment Guide
Thermage FLX for the jawline — the vector, the jowl, the timeline
An editorial reading of jawline-specific Thermage FLX in Gangnam: how senior operators plan the pull vector, manage the early jowl, calibrate the comfort pulse along the mandibular border, and what the four-month result actually looks like.
The jawline is the zone Thermage FLX is asked to do most of its work on, and it is also the zone where the procedure most often disappoints when the operator treats the face as a single field rather than as a sequence of vectors with distinct mechanical requirements. The editorial reading on the jaw — refined across post-procedure interviews with Hong Kong, Singapore, Taipei, and Tokyo patients — is that jawline outcomes correlate almost entirely with three operator decisions that happen before the first pulse: how the pull vector is planned, how the early jowl is managed, and how the comfort pulse is calibrated along the mandibular border. Patients arrive in Gangnam asking about shot count and tip generation; what actually predicts the result is the unglamorous geometry of where the operator places the grid, in what sequence, and against which anatomical landmark. What follows is the reading on jawline-specific Thermage FLX in Gangnam — the planning, the procedure, the recovery, and the four-month result that determines whether the trip was worth the flight.
The jawline reads as a vector, not a line
The jawline is, in editorial reading and in the senior physician's planning notes, a vector rather than a line. The phrase matters because it determines how the grid is laid before the procedure starts. The vector originates posteriorly at the angle of the mandible — the bony landmark just below and forward of the earlobe — and travels anteriorly along the mandibular border to the chin, with a critical inflection point where the parotid-masseteric fascia transitions into the lower cheek. A senior operator plans the pull along this vector before placing the first grid mark, and the grid is then oriented so the thermal contraction pulls along the vector rather than against it. Patients who watched the procedure planning on monitor often describe the marker lines as resembling a fishbone pattern radiating outward from the mandibular angle; this is the visual signature of vector-aligned planning. What this means practically: the shots are not distributed evenly across the lower face. The grid concentrates posteriorly at the mandibular angle (where the bony anchor allows the most mechanical purchase), tapers anteriorly along the border (where the soft tissue has progressively less anchor), and integrates with the cheek grid at the inflection point so the two zones pull as a coordinated field. The procedure performed without this vector planning — a uniform grid laid across the lower face — produces the result patients describe as flat or generally smoother but no shape change. The procedure performed with vector planning produces the result patients describe as the jawline came back.
Jowl management — the part most patients misunderstand
The early jowl is the soft-tissue descent along the anterior mandibular border that produces the visual reading of a softening jawline, and it is the single most common reason patients book Thermage FLX in Gangnam. What patients arrive expecting is a procedure that removes the jowl. What the procedure actually does, and what the editorial reading insists on naming clearly, is reorient and tighten the dermal scaffold that holds the jowl tissue in place. The distinction matters because the patients who arrive with the wrong expectation often conclude after four months that the procedure did not work — and what they mean is that the jowl is still visible, just less so. The honest reading on jowl-stage classification: an early jowl (mild anterior soft-tissue prominence, no pre-jowl sulcus, intact mandibular shadow) responds well to vector-aligned Thermage FLX with a 900-shot to 1200-shot face protocol and produces a visually durable reorientation across the four-month timeline. A moderate jowl (clearly visible pre-jowl sulcus, partial loss of the mandibular shadow, soft-tissue volume descent into the lower face) responds partially — the dermal tightening is real and the visual shift is measurable, but the procedure alone will not restore the jawline shape of an earlier decade. A late jowl (significant pre-jowl sulcus, marked soft-tissue ptosis, jowl tissue visibly draped over the mandibular border) is, in the senior physician's reading, outside the modality. Patients in this category are better served by a conversation about surgical or combination protocols rather than a single Thermage session. The most important consultation question for jowl-stage patients: which jowl-stage am I, and what specifically can the procedure do for me? The answer should be specific, not aspirational.
Comfort pulse on the mandibular border — why this matters
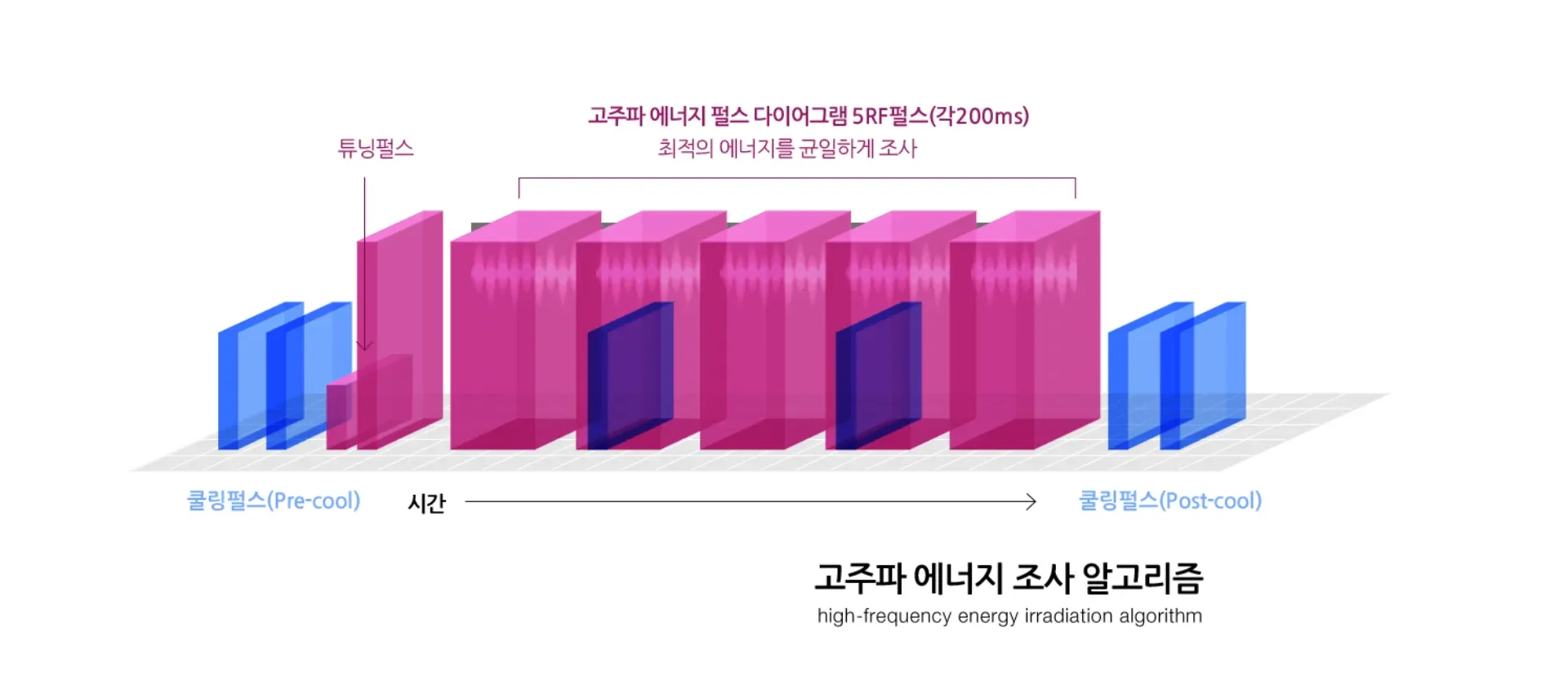
The mandibular border — the bony lower edge of the jawline — is the zone where pain perception during Thermage FLX is most pronounced, and it is also the zone where the operator must deliver the highest density of pulses to achieve a meaningful jawline contraction. The collision between these two facts is what the comfort pulse feature on the FLX generation handpiece is designed to resolve. The mechanism, in editorial reading: the handpiece delivers a brief vibratory stimulus immediately before the radiofrequency pulse, which engages the gate-control pain modulation pathway and meaningfully reduces the patient's perception of the thermal pulse that follows. The clinical literature describes this as a vibratory-assisted radiofrequency delivery system, and the practice-level reading on it is that the comfort pulse is the single most important reason patients tolerate the high-density mandibular grid required for a meaningful jawline result. Patients treated on earlier Thermage generations without the comfort pulse often reported the mandibular border as the procedure's most uncomfortable zone, and operators historically reduced shot density along this border to keep patients comfortable — at the cost of a weaker jawline result. The FLX generation comfort pulse allows the operator to deliver the full density grid along the mandibular border without compromising on comfort, which is the geometry that produces the meaningful jawline contraction over the four-month timeline. A consultation point worth raising: ask the operator how the comfort pulse cadence is calibrated for the mandibular border specifically. The answer should reference the patient's pain tolerance baseline, the soft-tissue density along the border, and the planned pulse density — not a generic clinic protocol.
Shot count, tip generation, and what the numbers actually mean for the jawline
The shot count question is the one patients ask first and the one that matters least in isolation. A 900-shot face protocol covers the full lower-third with appropriate jawline density for an early jowl presentation. A 1200-shot face protocol adds density to the mandibular border and the lateral cheek that integrates with it, and is the appropriate choice for moderate jowl presentations or for patients with denser facial tissue who require higher pulse density to achieve a meaningful thermal effect. The tip generation question is more important than the shot count question, and it is the one patients ask least. The Thermage FLX system delivers through a series of tip generations calibrated for specific anatomical zones — the standard face tip handles the cheek and lower face at appropriate dermal depth, the Total Tip 0.25 handles the periorbital zone at shallower depth, and the body tips handle the larger surface zones at greater pulse depth. For jawline work specifically, the standard face tip is the workhorse, and the senior operator's reading is that the question is less about tip generation and more about how the operator integrates the cheek grid with the mandibular grid so the two zones pull as a coordinated field. Patients arriving in Gangnam should ask about the integrated grid rather than the shot count — the shot count is the answer; the grid is the work.
The four-month timeline for jawline-specific Thermage FLX
The jawline result, like the broader Thermage FLX result, peaks at Month 3 to Month 4 after the procedure and persists for twelve to eighteen months in stable laxity progression. What the editorial reading insists on, for jawline patients specifically, is that the early visible reading at Day 7 to Week 2 is unrepresentative of the four-month result. The immediate thermal contraction produces a subtle reading that patients with baseline photographs sometimes notice and patients without baseline photographs rarely do. The early collagen response across Week 2 to Week 4 produces a measurable but modest jawline firming. The durable collagen remodelling across Week 4 to Month 4 produces the result that justifies the procedure — a visibly reoriented jawline that reads as a return of the mandibular shadow, a reduced pre-jowl sulcus, and a tighter dermal scaffold along the lower face. Patients should plan a four-month review with the senior physician, either on-site or remotely via the clinic coordinator, and the senior physician's reading at the four-month mark is the relevant data point for whether the procedure delivered for the specific jawline presentation. Earlier readings — at Day 7, at Week 2, at Week 6 — are premature and routinely undersell the eventual result.
Combining jawline Thermage FLX with adjacent modalities
Patients booking jawline-specific Thermage FLX in Gangnam often ask about combining the procedure with adjacent modalities — Ultherapy on the SMAS layer, microcurrent jaw protocols, regenerative bio-active sessions, or surgical thread lifts. The editorial reading on each combination, in brief. Ultherapy on the SMAS layer pairs well with Thermage FLX on the dermal layer for moderate jowl presentations where both layers contribute to the visible descent; the two modalities operate at different tissue depths and the senior physician's reading is that they can be sequenced on the same trip with a one-week to two-week interval between procedures. Microcurrent jaw protocols, where available, are a useful adjunct in the early recovery window and can be timed to support the collagen response across Week 2 to Week 4. Regenerative bio-active sessions — exosome boosters, growth-factor concentrates, polynucleotide injections — are typically scheduled in the Week 2 to Week 4 window to capitalise on the heating-induced bioavailability the literature suggests is real for combined protocols. Surgical thread lifts are a categorically different modality and are not typically combined on the same trip; a senior physician will sequence thread lift work after the four-month Thermage review rather than concurrently. The most important reading: combinations should be sequenced by the senior physician based on the specific jawline presentation, not assembled by the patient à la carte.
“The jawline is read as a vector, not a line — and patients who book the procedure understanding that distinction are almost always satisfied with the result.”
Editorial note
Frequently asked questions
How do I know if my jawline is a good candidate for Thermage FLX?
The honest reading depends on jowl stage. An early jowl with intact mandibular shadow and no pre-jowl sulcus is the strongest candidacy profile. A moderate jowl with visible pre-jowl sulcus responds partially and benefits from realistic expectations. A late jowl with significant soft-tissue ptosis is outside the modality and is better served by a different conversation. A senior physician consultation with on-site 3D imaging is the right way to classify your jowl stage rather than self-assessment from a mirror reading.
Will Thermage FLX give me a sharper jawline like surgery would?
No, and the editorial reading insists on naming this clearly. Thermage FLX tightens and reorients the dermal scaffold along the jawline, which produces a visually firmer reading and partial restoration of the mandibular shadow. It does not produce the structural shape change a surgical jawline contouring procedure does. Patients seeking surgical-level transformation are better served by a different consultation. Patients seeking durable non-surgical jawline maintenance are well served by Thermage FLX.
What shot count is right for jawline work specifically?
For an early jowl, a 900-shot face protocol with appropriate jawline density is generally sufficient. For a moderate jowl or denser facial tissue, a 1200-shot protocol with added density along the mandibular border and integrated cheek grid is the appropriate choice. The senior operator should calibrate shot count against your specific jowl-stage classification and facial tissue density rather than quote a generic number. Ask about the integrated grid rather than the shot count.
How painful is the jawline portion of the procedure?
The mandibular border is the procedure's most pain-sensitive zone. The comfort pulse feature on the FLX generation handpiece meaningfully reduces the perceived intensity through a vibratory pre-pulse mechanism. Most patients describe the jawline portion as a series of brief heating sensations rather than sharp pain. Patients with low pain tolerance should ask about adjusted pulse cadence and additional topical anaesthesia along the mandibular border specifically.
When will I see the jawline result after the procedure?
The early visible reading at Day 7 to Week 2 is unrepresentative. The durable result peaks at Month 3 to Month 4 after the procedure. Patients who took baseline photographs notice progressive jawline firming across Week 2 to Week 4 and a clearer reading at Month 2. The four-month review with the senior physician is the relevant data point. Earlier readings routinely undersell the eventual result, and patients who evaluate the procedure at Week 2 often conclude incorrectly that it did not work.
How long does the jawline result last?
Twelve to eighteen months in stable laxity progression. Patients with rapid laxity progression sometimes schedule a partial-coverage top-up at six months to consolidate the mandibular border specifically. Annual maintenance is the conventional planning baseline. The senior physician should set the retreatment cadence after the four-month review rather than commit a patient up front.
Can I combine jawline Thermage FLX with other procedures on the same trip?
Yes, with senior physician sequencing. Ultherapy on the SMAS layer pairs well for moderate jowl presentations with a one-week to two-week interval. Regenerative bio-active sessions are typically scheduled in the Week 2 to Week 4 window. Surgical thread lifts are not typically combined on the same trip and are sequenced after the four-month Thermage review. The combinations should be planned by the senior physician based on your specific presentation.
Is the jawline Thermage FLX procedure suitable for men?
Yes, and increasingly so. Male patients with early-to-moderate jowl presentations respond well to vector-aligned Thermage FLX, with the senior operator typically adjusting the grid geometry to preserve a stronger mandibular line rather than soften it. Male facial tissue tends to be denser and often benefits from a higher shot count protocol. Cultural reluctance to discuss non-surgical aesthetic work among regional male patients is real; consultation discretion is standard at Gangnam premium clinics.